Basics
Iron is an essential microelement that plays a role in many metabolic processes, particularly those associated with transporting oxygen and regulating cell growth and differentiation. In fact, iron is involved in well over 100 metabolic processes. Because the body cannot produce iron, it must be obtained from food. Iron deficiency is the most common nutrient deficiency worldwide. Iron deficiency develops gradually; it begins with a negative iron balance when dietary intake is insufficient to meet the body’s daily needs.
When an iron deficiency exists, the oxygen supply to cells is reduced, which can lead to impaired physical performance accompanied by tiredness and a weakened immune system. Other typical signs of iron deficiency are paleness, dry skin, brittle fingernails and a tendency to become overweight. High-risk groups include women in general, children and pregnant women; an estimated 22 percent of women in industrialized countries are affected. Up to 47 percent of all school-age children worldwide also develop some form of anemia, 25 percent of whom suffer from iron-deficiency anemia, the most severe kind of iron deficiency.
Effects
Iron, or more specifically iron salt, can exist in two forms: heme iron and non-heme iron. The former is derived from hemoglobin and is found in foods of animal origin. The latter is found in plant products, and is the form contained in nearly all dietary supplements or enriched foods. Unfortunately, non-heme iron is often more difficult for the body to absorb.
There are a multitude of factors that influence the body’s absorption of non-heme iron; for example, many foods and drinks contain ingredients that interfere with iron uptake. Therefore, it is always best to take iron supplements between meals. Some diseases and certain drugs can also inhibit iron absorption. Furthermore, different iron salts are more readily absorbed in different sections of the gastrointestinal tract.
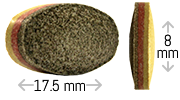
Unlike conventional food supplements which usually contain only one iron salt—typically iron —Ferrochron® is a unique formula that largely replaces iron sulfate with other more tolerable and bioavailable iron salts. By utilizing a triple-layer technology, the three iron salts in Ferrochron® are released in different sections of the gastrointestinal tract. This maximizes the advantages of each iron salt while also reducing side effects and greatly increasing bioavailability.
Ferrochron® tablet composition is as follows:
An initial outer layer immediately releases one-third of the iron in the upper digestive tract, starting in the stomach. This layer contains iron bisglycinate to guarantee an initial, rapid uptake in the upper digestive tract with maximum tolerability; these are properties that have been confirmed in various research studies.
After a short delay, an intermediate layer releases one-third of the iron in the form of iron sulfate. This occurs approximately one to two hours after taking the tablet, while it is being transported through the duodenum. At this state, vitamin C is also released to increase the bioavailability of this iron salt even further in this part of the intestine. The addition of vitamin C also helps to minimize any of the side effects that can occur from high doses of iron sulfate.
A third, extended-delay layer only starts to release its iron two to four hours after the tablet is ingested. At this time, the tablet is passing through the small intestine (from jejunum to ileum). This layer contains highly bioavailable, microencapsulated iron pyrophosphate coated with lecithin. This ensures maximum uptake of the remaining one-third of the iron as it passes through this part of the digestive tract, as has been confirmed in many studies.
By combining three iron salts, the amount of iron sulfate in Ferrochron® is reduced to an absolute minimum, thereby maximizing tolerability while at the same time ensuring high bioavailability of the entire iron content.
Uses
There are certain groups of people for whom iron deficiency is more common, and who could especially benefit from iron supplementation; for example, women who experience heavy menstruation. Pregnant and nursing women also tend to be iron-deficient. Nearly 18 percent of pregnant women in the United States suffer from iron-deficiency anemia; the consequences are often premature births or low birth weight. For this reason, supplementation is recommended during pregnancy, since it’s difficult to meet the body’s iron requirements through diet alone. Other groups at risk are women undergoing fertility treatments and children and adolescents whose iron requirements are higher during their growth phase. Men and women who suffer from Crohn’s disease, inflammatory bowel disease or coeliac disease, dialysis patients, extreme athletes and vegetarians are also known risk groups.
In order to reduce the risk of progressive iron deficiency in healthy people, the recommended daily doses of dietary iron are around 11 mg for infants between seven and twelve months old, 7 mg for children between the ages of one and three, 8 – 11 mg for children 4 years and older, 8 mg for men, 15 - 18 mg for adult women of childbearing age and at least 27 mg for pregnant women. If these amounts are not obtained every day or if large amounts are excreted each day, an iron deficiency or anemia will develop sooner or later. In these cases, higher supplemental doses are recommended.
Adults with a confirmed or suspected iron deficiency should take at least 30 – 60 mg of iron per day in addition to their normal diet, or even higher doses in severe cases. This supplementation should continue until the hemoglobin or ferritin levels, both measurable in the blood, have returned to normal. Ideally, by taking a chronobiologically designed supplement, the levels may be restored after about 12 – 16 weeks. People with a low-iron diet (e. g. vegans) or with a permanently higher need for iron intake (e. g. women with heavy menstrual bleeding, extreme athletes or those with a gastrointestinal condition) often require longer periods of supplementation.
Supplement Facts
Vitamin C (as Ascorbic Acid)
70 mg
78%
Iron (as Microencapsulated Ferric Pyrophosphate; as Ferrous Bisglycinate; as Ferrous Sulphate)
30 mg
167%
Other Ingredients: Microcrystalline cellulose (including hydroxypropylmethylcellulose and sodium carboxymethylcellulose), dicalcium phosphate, silicon dioxide, yellow iron oxide color, red iron oxide color.
Dosage: As a dietary supplement, take 1 tablet per day 120-30 minutes before your evening meal with 8 ounces of water. (Do not take with milk, coffee, alcohol or fruit juices.) For acute iron deficiency the dose can be increased to 2 tablets daily.
Caution: Do not exceed recommended dose. Pregnant or nursing mothers, children under 18, and individuals with a known medical condition should consult a physician before using this or any dietary supplement.